
Most people never think about their hips until something goes wrong. Then suddenly, every step hurts. Getting out of a chair feels like a chore. Walking to the kitchen or climbing a single flight of stairs becomes something you dread. You search online, read a hundred articles about hip joint pain and hip bone structure, and still feel confused about what is actually happening inside your body.
That confusion is understandable. The hip is one of the most complex joints in the human body. It involves bones, cartilage, multiple ligaments, dozens of muscles, fluid-filled sacs, nerves, and blood vessels, all working together so quietly that you only notice them when something breaks down. Hip pain causes range from simple muscle tightness to serious structural problems like avascular necrosis or fractures, and the location of your pain gives important clues about which part of the joint is affected.
This blog is a complete guide to hip anatomy written for patients, not textbooks. You will find clear explanations of hip bone anatomy, hip joint anatomy, the major hip muscles, how the hip joint works, and the most common problems that bring people to an orthopedic hip specialist. Whether you are dealing with a nagging ache in the groin, outer hip pain that keeps you awake at night, or stiffness that appeared after sitting at a desk for years, this guide will help you make sense of what your body is telling you.
Understanding your hip anatomy is also the first step toward having a more informed conversation with your doctor. When you know the difference between the acetabulum and the femoral head, or between trochanteric bursitis and hip osteoarthritis, you are better placed to ask the right questions and understand the treatment options available to you, whether that means physiotherapy, injections, or hip replacement surgery.
What Is the Hip Joint?
The hip is the second largest joint in the human body, just behind the knee. It connects your thigh bone (femur) to your pelvis and carries your entire body weight with every step you take.
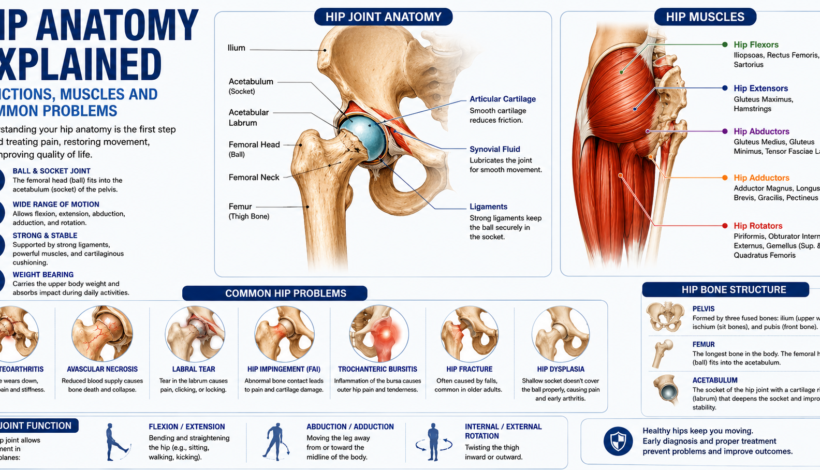
The hip joint is a ball and socket joint. The rounded top of the femur, called the femoral head, fits into a cup-shaped socket in the pelvis called the acetabulum. This design gives your hip a wide range of movement while keeping it secure enough to bear hundreds of kilograms of force.
The articular cartilage lining the femoral head and the acetabulum is about 6 mm thick at its deepest point. It is extremely smooth and kept lubricated by synovial fluid, which reduces friction so the joint glides cleanly during movement. When this cartilage wears down, pain starts.
Hip Bone Structure: The Bones of the Hip Joint
Understanding hip bone anatomy starts with knowing which bones form the joint and surrounding pelvis and hip anatomy.
The Pelvis
Three bones fuse together to form the pelvic bone on each side:
- Ilium is the large, wing-shaped upper section. When you put your hands on your hips, you are actually resting them on the ilium.
- Ischium forms the lower and back portion. The bony points you sit on are called the ischial tuberosities or “sit bones.”
- Pubis is the front section. Both sides meet at the pubic symphysis.
The Femur
The femur or thigh bone is the longest bone in the body. At its top sits the femoral head, the ball that fits into the acetabulum. Just below is the femoral neck, which connects the head to the shaft. The greater trochanter is the bony bump on the outside of your hip that you can feel with your hand. Many muscles attach to it.
The Acetabulum
The acetabulum is the socket of the hip joint. It faces outward and slightly downward, which is why the leg hangs at a slight angle. Around its rim is a ring of fibrocartilage called the acetabular labrum. The labrum deepens the socket, improves stability, and seals in synovial fluid to keep the joint lubricated.
Hip Joint Anatomy: Ligaments and Cartilage
The hip joint anatomy includes several strong ligaments that hold the ball inside the socket.
Iliofemoral Ligament (Y Ligament of Bigelow)
This is the strongest ligament in the entire human body. It runs across the front of the hip joint and stops the hip from bending backwards past its normal limit. Without it, simply standing upright would put enormous strain on the hip.
Pubofemoral Ligament
Located on the lower front of the joint, it limits how far the leg can swing outward and prevents excessive extension.
Ischiofemoral Ligament
This wraps around the back of the hip joint. It is the weakest of the three and helps check excessive rotation and extension.
Articular Cartilage
Cartilage is the smooth white tissue covering the bones inside the joint. It has no blood supply of its own, which is why it heals slowly once damaged. The cartilage absorbs shock and allows bones to glide without friction.
Synovial Membrane and Fluid
A soft lining called the synovial membrane lines the joint capsule. It produces synovial fluid, which acts as a natural lubricant. Healthy joints have just enough fluid to keep things moving smoothly. Inflammation can cause the membrane to produce too much fluid, resulting in joint swelling and stiffness.
Hip Muscle Anatomy: The Muscles That Move and Protect the Hip
The hip joint is surrounded by some of the largest and most powerful muscles in the body. These muscles do not just create movement. They protect the joint by controlling loads passing through it.
Hip Flexors
These muscles lift the thigh toward the chest, which happens every time you take a step.
- Iliopsoas is the primary hip flexor. It consists of the psoas major and the iliacus, which join at the groin and attach to the lesser trochanter of the femur. People who sit for long hours at a desk often have tight, shortened iliopsoas muscles, which can tilt the pelvis forward and cause lower back pain.
- Rectus Femoris is part of the quadriceps group but also crosses the hip joint to assist with hip flexion.
- Sartorius is the longest muscle in the body, running from the hip crest diagonally across the thigh to the inner knee.
Hip Extensors
These muscles drive the leg backward, powering walking, running, and stair climbing.
- Gluteus Maximus is the largest muscle in the body. It drives powerful movements like standing up from a chair, climbing stairs, and running uphill.
- Hamstrings (biceps femoris, semitendinosus, semimembranosus) cross both the hip and knee joints. They extend the hip and flex the knee simultaneously.
Hip Abductors
These muscles move the leg away from the body’s midline. More importantly, they stabilize the pelvis when you stand on one leg, which happens during every walking step.
- Gluteus Medius sits on the outer pelvis and is probably the most important stabilizing muscle around the hip. Weakness here causes the pelvis to drop toward the opposite side during walking, a pattern called a Trendelenburg gait.
- Gluteus Minimus lies underneath the gluteus medius and works alongside it.
- Tensor Fasciae Latae (TFL) connects into the iliotibial band, a thick band of tissue running down the outside of the thigh to the knee.
Hip Adductors
These muscles pull the leg back toward and across the midline.
- Adductor Magnus, Longus, and Brevis form the main group along the inner thigh.
- Gracilis is a thin muscle running from the pubic bone down to the inner knee.
- Pectineus sits at the top of the inner thigh and assists with both adduction and hip flexion.
Hip Rotators
Deep rotator muscles control inward and outward turning of the thigh. The six deep rotators are the piriformis, obturator internus, obturator externus, gemellus superior, gemellus inferior, and quadratus femoris. The piriformis is the most well known because it sits near the sciatic nerve. When it becomes tight or inflamed, it can compress the nerve and cause pain that travels down the leg, a condition sometimes called piriformis syndrome.
Hip Joint Function: What Your Hips Actually Do
The hip joint allows movement in three planes:
- Flexion and Extension: Bending and straightening the hip, as in sitting, squatting, walking, and kicking.
- Abduction and Adduction: Moving the leg outward and inward, needed for side steps and balance.
- Internal and External Rotation: Twisting the thigh inward and outward, needed for changing direction and sports movements.
Beyond movement, the hip transmits load from the upper body to the legs. Every time you stand, the hip absorbs forces equal to roughly 2.5 to 3 times your body weight. During running, those forces rise to 5 to 8 times body weight. The bones, cartilage, ligaments, muscles, and bursae all share this load together.
Bursae deserve a mention here. These are small, fluid-filled sacs placed at friction points around the joint, particularly between muscles, tendons, and bony surfaces. The trochanteric bursa over the greater trochanter is the one most commonly inflamed in people with outer hip pain.
Common Hip Problems: Causes, Symptoms, and When to Worry
Hip Osteoarthritis
This is the most common hip problem in adults over 50. Osteoarthritis of the hip occurs when the articular cartilage gradually wears away. The femoral head and acetabulum begin to rub against each other, leading to pain, stiffness, and eventually loss of movement.
Early symptoms include a dull ache in the groin or thigh after activity, stiffness after sitting for a while, and reduced range of motion. As cartilage loss progresses, pain occurs even at rest and during the night.
Risk factors include age, obesity, previous hip injury, and family history. Hip osteoarthritis is a leading reason for hip replacement surgery.
Hip Fracture
Hip fractures most often occur in older adults after a fall, though high-energy injuries like road accidents can cause them at any age. The femoral neck and the intertrochanteric region (just below the femoral neck) are the two most common fracture sites. Hip fractures in elderly patients are serious medical events with significant complications if not treated promptly. Most require surgery.
Avascular Necrosis (AVN) of the Hip
Also called osteonecrosis, AVN occurs when the blood supply to the femoral head is disrupted. Without adequate blood flow, bone cells die. The femoral head can collapse over time, leading to severe arthritis.
Causes of AVN include long-term steroid use, heavy alcohol consumption, sickle cell disease, previous hip dislocation, and some blood disorders. The condition is more common in younger adults than osteoarthritis. Early diagnosis before femoral head collapse gives patients a much better chance of preserving the joint.
Hip Labral Tear
The acetabular labrum can tear due to repetitive movement, impingement (when the bones rub abnormally), or trauma. Athletes in sports involving repeated hip flexion, such as football and cricket, are at higher risk.
Symptoms include a catching or clicking sensation inside the hip, groin pain with prolonged sitting, and reduced range of motion. Many labral tears are found on MRI scans in patients who were initially thought to have a muscle strain.
Hip Impingement (Femoroacetabular Impingement or FAI)
FAI occurs when there is abnormal contact between the femoral head and the acetabulum. This happens because of extra bone growth (a CAM lesion on the femoral head, or a PINCER lesion on the acetabular rim, or both together). Over time, this repetitive abnormal contact damages the cartilage and labrum.
FAI is increasingly recognised as a cause of hip pain in young and middle-aged active people. Symptoms include groin pain during flexion activities, reduced internal rotation, and pain after prolonged sitting.
Hip Bursitis
The trochanteric bursa on the outer hip is the most commonly inflamed. Trochanteric bursitis causes pain on the outer side of the hip that worsens with lying on that side, climbing stairs, or standing for long periods. It often develops from overuse, direct trauma, or muscle tightness from the IT band.
Hip Muscle Strains and Tendinopathy
Sudden overstretching of hip muscles causes strains, most commonly in the hip flexors, hamstrings, or adductors. Athletes who sprint, kick, or change direction quickly are most at risk. Tendinopathy refers to chronic degeneration of the tendons attaching these muscles to bone, causing pain that comes on gradually with repeated activity.
Hip Dysplasia
Hip dysplasia means the acetabulum is too shallow and does not adequately cover the femoral head. It may be diagnosed at birth or discovered in adulthood when it causes hip pain, labral tears, or early arthritis. Some cases require surgical correction to restore normal joint mechanics.
Hip Pain Causes: How to Read Your Symptoms
| Location of Pain | Likely Cause |
| Groin / front of hip | Hip joint problem (arthritis, labral tear, FAI, iliopsoas tendon) |
| Outer hip / greater trochanter | Trochanteric bursitis, gluteus medius tendinopathy |
| Buttock / back of hip | Piriformis syndrome, sacroiliac joint problem, referred pain from spine |
| Inner thigh | Adductor strain, obturator nerve problem |
| Thigh, knee, or lower leg | Referred pain from hip joint, sciatic nerve involvement |
Pain that is worse with activity and better with rest usually points to a structural joint problem or tendon issue. Pain that wakes you at night or is present constantly at rest needs prompt evaluation. Pain in the groin after a minor fall in someone over 60 should be investigated for a hip fracture immediately.
Hip Replacement Anatomy: What Changes After Surgery
In a total hip replacement (total hip arthroplasty), the damaged femoral head and the worn acetabulum are replaced with prosthetic components. A metal or ceramic femoral stem is fixed into the femur. A metal cup is placed into the acetabulum with a smooth liner inside it. A new femoral head, usually ceramic or metal, attaches to the stem and articulates with the liner.
Modern implants last 15 to 20 years or longer in most patients. Understanding hip replacement anatomy helps patients know what to expect during recovery and why certain precautions (like avoiding deep hip flexion in the early weeks) are given.
When to See an Orthopedic Hip Specialist
Many people wait too long before getting their hip assessed. Here are situations where early review matters:
- Hip pain that has lasted more than 4 to 6 weeks without improvement
- Pain that limits walking distance, climbing stairs, or daily activity
- A grinding or locking sensation inside the hip
- Hip stiffness in the morning lasting more than 30 minutes
- Groin or hip pain in a young or middle-aged person with no clear cause
- Any hip pain after a fall or injury, especially in adults over 60
- Pain suspected to be AVN, given the importance of early intervention before femoral head collapse
A specialist can order the right imaging (X-ray, MRI, or CT) to identify the exact problem and recommend appropriate hip treatment options, ranging from physiotherapy and injections to keyhole surgery or joint replacement.
Hip Pain Treatment in Mumbai
If you are dealing with persistent hip joint pain, stiffness, or a suspected injury, early diagnosis and proper treatment can prevent things from getting worse. Dr. Abhay Chhallani is an orthopedic hip specialist in Mumbai who provides expert evaluation and treatment for the full range of hip conditions, including hip arthritis, AVN, labral tears, FAI, hip fractures, and hip replacement surgery.
Getting the right diagnosis sooner means more treatment options and, often, a better outcome.
Key Takeaways
- The hip joint is a ball and socket joint formed by the femoral head (femur) and the acetabulum (pelvis).
- Hip bone structure includes the ilium, ischium, pubis, femoral head, and acetabulum.
- Major hip muscles include the iliopsoas, gluteus maximus, gluteus medius, hamstrings, adductors, and deep rotators like the piriformis.
- The hip joint allows flexion, extension, abduction, adduction, and internal and external rotation.
- Common hip problems include osteoarthritis, AVN, labral tears, FAI, bursitis, hip fractures, and dysplasia.
- Hip pain location gives useful clues: groin pain usually means a joint problem, outer hip pain often means bursitis or gluteal tendinopathy.
- Consult a hip specialist if pain persists beyond 4 to 6 weeks or significantly limits your daily movement.
For expert hip diagnosis and hip pain treatment in Mumbai, consult Dr. Abhay Chhallani. Early evaluation leads to better outcomes for all hip conditions, from conservative management to advanced hip replacement surgery.
Frequently Asked Questions About Hip Anatomy and Hip Pain
What are the main bones of the hip joint?
The hip joint is formed by two main bones: the femoral head (the ball at the top of the thigh bone) and the acetabulum (the cup-shaped socket in the pelvis). The pelvis itself is made up of three fused bones called the ilium, ischium, and pubis.
What type of joint is the hip?
The hip is a ball and socket joint. This design allows movement in multiple directions, including flexion, extension, abduction, adduction, and rotation, making it one of the most mobile joints in the body.
What causes hip joint pain?
Hip joint pain has many causes. The most common include osteoarthritis, trochanteric bursitis, labral tears, hip impingement (FAI), avascular necrosis, hip fractures, muscle strains, and referred pain from the lower back or sciatic nerve. The location of the pain, whether groin, outer hip, or buttock, helps identify the cause.
What are the hip muscles responsible for?
Hip muscles control all movement at the joint and stabilize the pelvis during walking and standing. The main groups are hip flexors (iliopsoas, rectus femoris), hip extensors (gluteus maximus, hamstrings), hip abductors (gluteus medius, gluteus minimus), hip adductors (adductor longus, magnus, brevis), and hip rotators (piriformis and the five other deep rotators).
What is the acetabulum?
The acetabulum is the socket of the hip joint, located on the outer surface of the pelvis. It is a deep, cup-shaped cavity that receives the femoral head. Around its rim sits the acetabular labrum, a ring of fibrocartilage that deepens the socket and helps seal in lubricating synovial fluid.
What is avascular necrosis of the hip?
Avascular necrosis (AVN) of the hip happens when the blood supply to the femoral head is cut off or reduced. Without adequate blood flow, bone tissue dies and the femoral head can collapse over time. It is often caused by steroid use, alcohol, hip dislocation, or blood disorders. Early diagnosis is very important because catching it before femoral head collapse gives far more treatment options.
What is hip replacement surgery?
A total hip replacement (total hip arthroplasty) is a procedure in which the worn-out femoral head and the damaged acetabulum are replaced with artificial components. The surgery relieves pain and restores mobility in patients with severe hip osteoarthritis, advanced AVN, or other end-stage hip conditions. Modern implants typically last 15 to 20 years or more.
When should I see an orthopedic hip specialist?
See a specialist if your hip pain has lasted more than 4 to 6 weeks, limits daily activities, is associated with a grinding or locking sensation, wakes you at night, or follows a fall or injury. In Mumbai, Dr. Abhay Chhallani provides complete diagnosis and hip treatment options for all hip conditions.
What is the iliofemoral ligament?
The iliofemoral ligament, also called the Y ligament of Bigelow, is the strongest ligament in the human body. It runs across the front of the hip joint and prevents the hip from bending backward beyond its normal range, which is why we can stand upright without muscular effort.
Can hip pain come from the lower back?
Yes. The sciatic nerve originates in the lower spine and travels through the buttock region close to the piriformis muscle before running down the leg. Problems in the lumbar spine, such as a disc herniation, can cause pain that feels like it is coming from the hip or buttock. This is why a proper clinical examination and correct imaging are needed to identify the true source of pain.
